Have you ever woken up in the middle of the night with your big toe feeling like it’s on fire? This intense pain is often a hallmark of gout, a painful form of arthritis that affects about 1-2% of adults. Finding effective Gout Treatment in Mohali is the first step toward lasting relief. Historically known as “the disease of kings,” gout has actually become more common in recent decades.
Gout occurs when urate crystals accumulate in your joints, causing inflammation and intense pain during an attack. This condition most commonly affects your big toe joint, though it can target other joints as well. High uric acid levels in your body are the primary culprit, often resulting from eating or drinking foods high in purines. Additionally, certain risk factors increase your likelihood of developing gout, including being overweight, having high blood pressure, diabetes, kidney disease, or heart failure. Men are three times more likely to develop this condition than women, though anyone can be affected.
Fortunately, with early diagnosis, appropriate treatment, and lifestyle changes, gout is one of the most controllable forms of arthritis. In this comprehensive guide, Dr. Manu Mengi explains everything you need to know about managing and preventing gout flares.
> > > CTA: Is your big toe swollen and red? Don't ignore the signs. Consult with Dr. Manu Mengi, a leading Red Painful Toe Specialist in Mohali, for an accurate diagnosis. Book your appointment today: +91 87250 11661
Understanding Gout: What It Is and How It Starts
Gout represents a complex form of inflammatory arthritis that occurs when sharp, needle-shaped crystals form in and around your joints. These crystals cause intense inflammation, resulting in sudden attacks of severe pain, swelling, and tenderness.
What is gout and how it affect joints
Gout is characterised by the formation of monosodium urate (MSU) crystals in joints and surrounding tissues. These crystals trigger highly inflammatory responses in the affected areas. The inflammation doesn’t just cause pain—it can eventually lead to joint damage if left untreated. Furthermore, gout progresses through several stages, beginning with asymptomatic hyperuricemia, followed by acute gout flares, intervals between attacks, and eventually, in some cases, chronic gout with tophi (crystal deposits under the skin).
The role of uric acid and purines
At the heart of gout is uric acid, the final product of purine metabolism. Purines are chemicals naturally found in your body and certain foods. Normally, uric acid dissolves in your blood and passes through your kidneys into urine. However, problems arise in two scenarios: either your body produces too much uric acid, or your kidneys don’t excrete enough.
Consequently, uric acid can build up in your bloodstream—a condition called hyperuricemia. When levels exceed 6.8 mg/dL (the saturation threshold), uric acid can form those painful MSU crystals. Essentially, these crystals are what cause the inflammation and intense pain of a gout attack.
Why the big toe is often the first target
The first metatarsophalangeal joint (your big toe joint) is ground zero for approximately 50% of initial gout attacks, with about 90% of patients experiencing at least one attack in this location. This preference for the big toe isn’t random—there are scientific reasons behind it.
Temperature plays a significant role in crystal formation. A reduction of even 2°C is sufficient to lower the solubility point of urate from 6.8 to 6.0 mg/dL. The big toe, being farther from your body’s core and having less tissue coverage, naturally maintains a slightly lower temperature. Additionally, this joint experiences repetitive trauma from walking, creating an ideal environment for crystal formation.
Unlike other forms of arthritis, gout is largely controllable with proper management of uric acid levels. Understanding this connection between uric acid and gout symptoms is the first step toward effective treatment.
> > > CTA: Struggling with high uric acid? Get personalised advice from the Best Gout Doctor in Mohali. Dr. Mengi creates tailored management plans to prevent crystal formation and stop the pain. Call now: +91 87250 11661
Recognising the Signs: Symptoms and Triggers
The sudden, excruciating pain of a gout attack often strikes without warning, leaving you searching for relief in the middle of the night. Recognising the symptoms early can help you seek treatment promptly and potentially reduce the severity of flares.
Gout symptoms in the foot and other joints
While the big toe is gout’s favourite target, the condition doesn’t limit itself to just one location. Gout can also affect your ankles, knees, elbows, wrists, and fingers. The pain is typically most severe within the first 4-12 hours after it begins. As gout progresses, you might experience a limited range of motion in the affected joints.
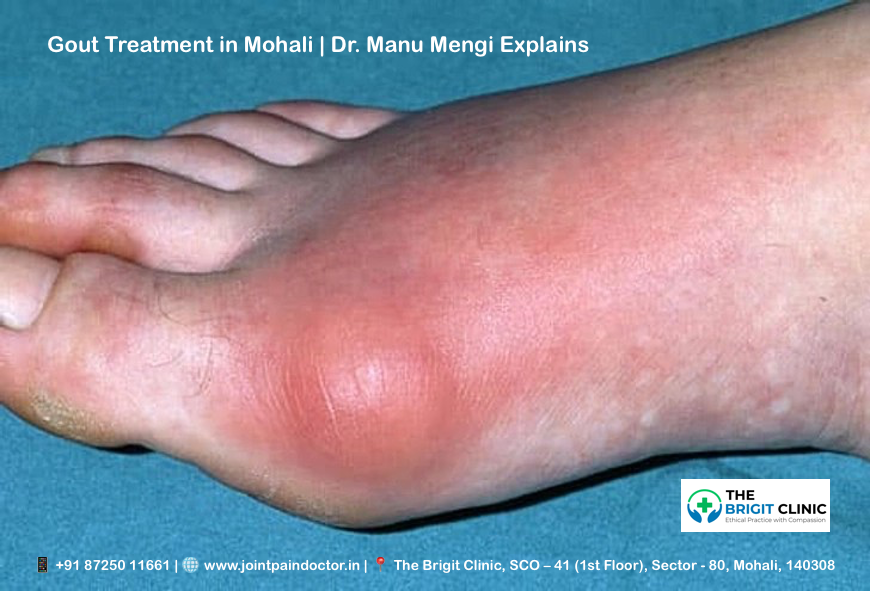
Swollen big toe joint and severe tenderness
The joint at the base of your big toe often bears the brunt of a gout attack. During a flare, this joint becomes so tender that even the light touch of a bedsheet can cause excruciating pain. You’ll notice significant swelling along with this tenderness, making it difficult to wear shoes or walk normally.
Redness & heat in joints during a flare
Beyond pain and swelling, visual cues help identify a gout attack. The affected joint typically becomes noticeably red or discoloured. Moreover, you’ll feel warmth or even a sensation like the joint is “on fire”. This inflammation is your body’s response to the sharp urate crystals irritating the joint.
Gout attack signs and how long they last
Gout flares often begin suddenly at night, with pain intense enough to wake you from sleep. A typical gout attack lasts between one and two weeks. Between flares, you usually won’t experience any symptoms. Nevertheless, without proper treatment, attacks may become more frequent and last longer over time.
Alcohol binge and other common triggers
Research shows alcohol consumption is the most common trigger for gout attacks, responsible for 14% of flares in one study. Specifically, drinking more than one alcoholic beverage in a day raises your risk of experiencing a gout attack. Beer appears to pose a greater risk than spirits, due to its high purine content.
Other common triggers include:
- Consuming red meat or seafood
- Dehydration
- Physical injury or excessive activity
- Extremely warm or cold weather
For those with gout, experts recommend avoiding alcoholic beverages entirely, despite the potential benefits of moderate consumption for other health conditions.
> > > CTA: Woken up by a sudden, fiery joint pain? You don't have to suffer through a gout flare alone. Contact Dr. Manu Mengi's Clinic in Mohali for urgent consultation and effective pain relief strategies.
What Causes Gout: Risk Factors and Underlying Conditions
Understanding what causes gout begins with identifying its root mechanism – disrupted uric acid balance in your body. Let’s explore the factors that put you at risk.
High uric acid levels and hyperuricemia
Hyperuricemia occurs when uric acid levels exceed 6.8 mg/dL in your blood. This condition happens when your body either produces too much uric acid or your kidneys don’t excrete enough. Although one-quarter of people with hyperuricemia develop gout, most remain symptom-free.
Risk factors for gout – diet, alcohol, obesity
Your dietary choices significantly impact gout risk. Foods high in purines, such as red meat, organ meats, and certain seafood, can raise uric acid levels. Beer consumption poses a greater risk than other alcoholic beverages because of its high guanosine content. Weight gain is another major factor – obesity increases your risk of gout by 3.26 times compared to a normal weight.
Genetics & gout: family history matters
Gout runs in families, with heritability estimated at approximately 60%. About 20% of people with gout have a relative with the condition. Research shows that an additive genetic score of high-risk alleles can increase gout risk up to 41-fold.
Medications that trigger gout
Certain medications raise uric acid levels in your blood. Diuretics increase the relative risk of gout by almost 80%. Other culprits include low-dose aspirin, cyclosporine, and some transplant medications.
Hormonal changes in gout (e.g., menopause)
For women, menopause significantly increases gout risk. The hormone estrogen helps eliminate uric acid through urine. After menopause, estrogen production declines, causing uric acid levels to rise.
Gout & kidney disease: a two-way link
A bidirectional relationship exists between gout and kidney disease. Kidney disease impairs uric acid excretion, raising gout risk. Conversely, high uric acid can damage the kidneys by forming stones and causing scarring.
> > > CTA: Confused about how your diet or medications affect your gout? Get a personalised Uric Acid Diet Consultation in Mohali with Dr. Mengi to understand your triggers and build a prevention plan.
Diagnosis and Treatment Options Explained
Getting an accurate diagnosis is crucial for effective gout management. Modern diagnostic techniques have improved physicians’ ability to detect and monitor this painful condition.
Ultrasound for gout detection
Ultrasound has emerged as a valuable tool for diagnosing gout, offering high-resolution imaging without radiation. The characteristic “double contour sign” (an irregular hyperechoic line over cartilage) has 43.7% sensitivity but 99% specificity for gout. Ultrasound can also identify tophaceous deposits in soft tissues and joints that might not be evident during clinical examination.
X-ray changes in chronic gout
X-rays typically show normal findings early in the disease. In chronic gout, hallmark features include marginal erosions with overhanging edges and sclerotic margins. Soft-tissue nodules (tophi) may appear as dense masses with higher attenuation than surrounding tissues.
Corticosteroids in gout treatment
Corticosteroids effectively treat acute gout flares, especially for patients who cannot tolerate NSAIDs. Options include oral prednisone (30-40mg daily for 5 days), intravenous administration, or direct joint injections. For single-joint gout, intra-articular injections offer fewer systemic side effects.
Gout treatment without medications
Non-pharmaceutical approaches include applying ice to affected joints, resting the inflamed area, and drinking plenty of water. Maintaining a healthy weight through regular exercise helps prevent flares, with low-impact activities like walking or swimming being ideal.
Managing chronic gout vs acute gout
Acute gout requires rapid inflammation control within 24 hours of symptom onset. Chronic gout management focuses on lowering serum uric acid below 6 mg/dL through long-term therapy. This distinction is essential—treating inflammation during flares differs from preventing future attacks through urate-lowering strategies.
> > > CTA: Need a precise diagnosis? As a leading Uric Acid Treatment Doctor in Mohali, Dr. Mengi uses advanced ultrasound imaging to accurately detect gout crystals and create a targeted treatment strategy for both acute and chronic gout. Visit our clinic to know more.
Conclusion
Gout, while extremely painful, remains one of the most manageable forms of arthritis when properly addressed. Understanding the connection between uric acid levels and gout attacks enables you to take control of this condition. Certainly, the buildup of urate crystals causes those excruciating flares, but knowledge about triggers like alcohol consumption, purine-rich foods, and certain medications gives you the power to prevent attacks.
Therefore, working closely with healthcare providers becomes essential for proper diagnosis and treatment. Advanced diagnostic tools, such as ultrasound, can detect gout even before visible symptoms appear. After diagnosis, treatment options range from medications that reduce inflammation during acute attacks to long-term strategies for lowering uric acid levels below the crystal-forming threshold.
Besides medical interventions, lifestyle modifications play a crucial role in gout management. Weight loss, adequate hydration, and avoiding high-purine foods significantly reduce your risk of future flares. Additionally, limiting alcohol consumption, particularly beer, helps maintain lower uric acid levels.
Remember that gout management requires both immediate relief during attacks and ongoing prevention between episodes. Though historically called “the disease of kings,” gout does not have to rule your life. With early detection, appropriate treatment, and consistent lifestyle adjustments, you can effectively manage this condition and maintain joint health for years to come.
Key Takeaways
Understanding gout empowers you to manage this painful but controllable form of arthritis effectively through proper diagnosis, treatment, and lifestyle modifications.
• Gout occurs when uric acid crystals form in joints, most commonly affecting the big toe first due to lower temperature and repetitive trauma from walking.
• Alcohol consumption is the top trigger for gout attacks, with beer posing a higher risk than other alcoholic beverages due to its purine content.
• Early diagnosis using ultrasound and X-rays enables targeted treatment, distinguishing between acute flare management and chronic prevention strategies.
• Lifestyle changes like weight loss, hydration, and avoiding high-purine foods significantly reduce attack frequency and severity.
• Gout is highly manageable when uric acid levels stay below 6 mg/dL through medication, diet modifications, and consistent medical monitoring.
With proper understanding of triggers, symptoms, and treatment options, gout doesn’t have to control your life. The key lies in working with healthcare providers to develop a comprehensive management plan that addresses both immediate pain relief and long-term prevention strategies.
> > > CTA: Ready to take control of your gout? Partner with Dr. Manu Mengi Gout Specialist Mohali, for a comprehensive management plan that combines advanced treatment with sustainable lifestyle changes. Your journey to a pain-free life starts here.
FAQs
Q1. What exactly is gout, and how does it affect the body?
A1. Gout is a form of inflammatory arthritis caused by the buildup of uric acid crystals in joints, most commonly in the big toe. It results in sudden attacks of severe pain, swelling, and tenderness. Gout occurs when the body either produces too much uric acid or the kidneys don’t excrete enough, leading to crystal formation in joints.
Q2. What are the most common triggers for a gout attack?
A2. The most common trigger for gout attacks is alcohol consumption, particularly beer, due to its high purine content. Other triggers include consuming red meat or seafood, dehydration, physical injury, and extreme weather conditions. Avoiding these triggers, especially limiting alcohol intake, can help reduce the frequency of gout flares.
Q3. How can I quickly relieve gout symptoms at home?
A3. To quickly relieve gout symptoms at home, apply ice to the affected joint, rest the inflamed area, and drink plenty of water. Some people find cherry juice helpful in reducing uric acid levels. However, it’s important to consult with a healthcare provider for proper treatment, as these methods provide temporary relief but don’t address the underlying cause.
Q4. Are there any non-medication approaches to managing gout?
A4. Yes, there are several non-medication approaches to managing gout. These include maintaining a healthy weight through regular low-impact exercise like walking or swimming, staying well-hydrated, and avoiding foods high in purines. Lifestyle modifications play a crucial role in preventing gout flares and managing the condition long-term.
Q5. How is gout diagnosed, and what treatment options are available?
A5. Gout is typically diagnosed through a combination of clinical symptoms, blood tests to measure uric acid levels, and imaging techniques like ultrasound or X-rays. Treatment options include medications to reduce inflammation during acute attacks, such as NSAIDs or corticosteroids, and long-term therapies to lower uric acid levels. The goal is to bring serum uric acid below 6 mg/dL to prevent future attacks and complications.
Dr. Manu Mengi – Gout Specialist Mohali
If you are looking for expert and compassionate care for gout in Mohali, look no further than Dr. Manu Mengi. Renowned as one of the Best Orthopedic Doctors in Chandigarh Mohali, Dr. Manu Mengi specialises in the diagnosis and management of gout and other joint pain disorders. His patient-centric approach combines cutting-edge diagnostic technology with evidence-based treatment protocols to provide both immediate relief and long-term prevention strategies. Whether you’re experiencing your first painful flare or struggling with chronic gout, Dr. Mengi and his team are dedicated to helping you regain your mobility and live a pain-free life. Schedule a consultation at his Mohali clinic to begin your journey toward effective gout management.
Book Appointment - Call Us: +91 87250 11661 | Find Our Clinic: Get Directions

Dr. Manu Mengi is a best orthopedic doctor in Mohali, specializing in joint pain, arthritis, and sports injuries. With qualifications in orthopedics and advanced training in joint replacement, he provides effective care for bone and joint conditions, helping patients improve mobility and manage pain with the right treatment approach.